

Charles R. Goulding and Andress Bonafe break down how Boston Scientific and Johnson & Johnson’s EP rivalry is fueling explosive PFA growth and a surge in demand for 3D printed cardiac models.
Boston Scientific and Johnson & Johnson have turned electrophysiology (EP) into one of MedTech’s hottest arenas. On October 22, 2025, Boston Scientific reported third-quarter electrophysiology sales of US$865 million, up about 64% year-over-year, propelled by its FARAPULSE ablation system. The 64% increase is almost unheard of in most industries. The company has signaled that it is aiming for EP leadership, while Johnson & Johnson’s Biosense Webster has made clear that it expects to hold the lead and is “not rolling over.” For additive manufacturing, the implication is clear: the push for speed and precision in ablation is increasing demand for 3D printed cardiac anatomical models used for planning, training, and procedure simulation.
Understanding Electrophysiology and Modern Ablation Approaches
Electrophysiology, or EP, is the branch of cardiology that focuses on the heart’s electrical system. When the electrical signals fire incorrectly, the heartbeat can be too fast, too slow, or irregular, a group of problems known as arrhythmias. EP testing uses thin catheters inside the heart to locate where abnormal rhythms begin so clinicians can plan treatment.
A common treatment is catheter ablation. Traditional ablation uses energy to destroy small areas of tissue that trigger the arrhythmia. Radiofrequency ablation applies heat, and cryoablation applies very cold temperatures. The choice depends on the patient’s specific rhythm problem.
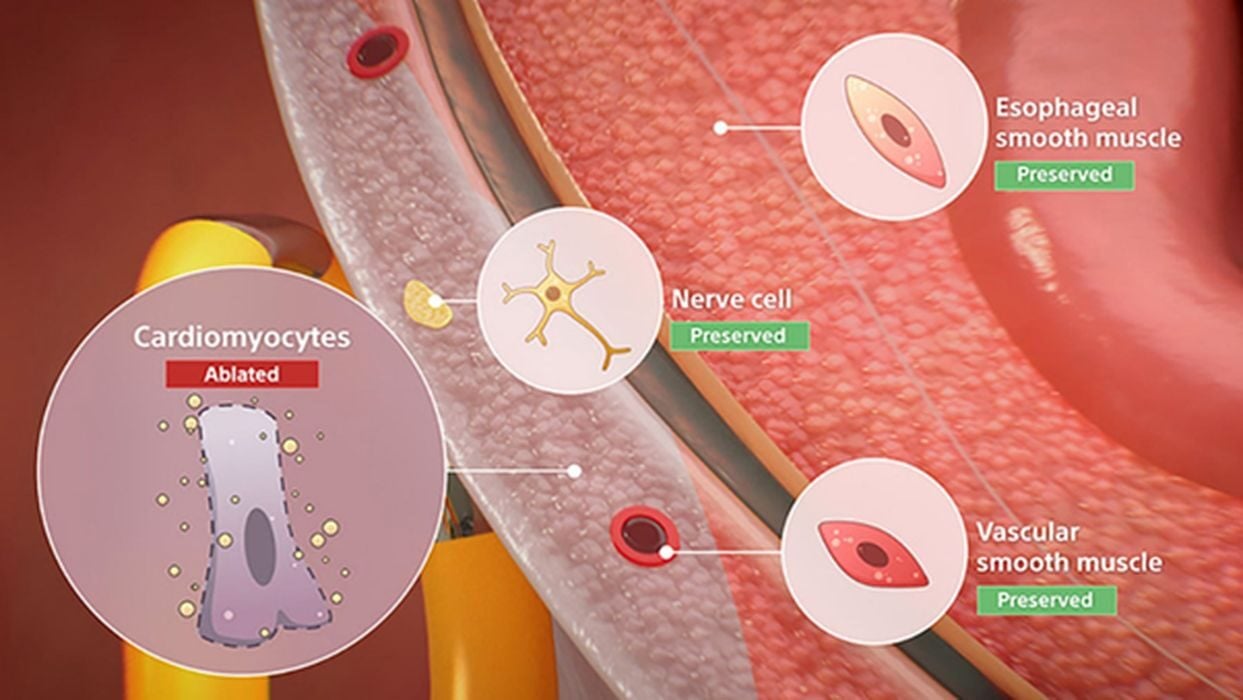
A newer approach is pulsed field ablation, or PFA. PFA delivers very short electrical pulses that create irreversible electroporation in targeted cells. Because it is non-thermal, PFA is designed to affect the arrhythmia source while limiting impact on nearby structures. Reviews and clinical studies describe PFA as an effective alternative to thermal ablation for atrial fibrillation.
FARAPULSE and VARIPULSE: How the Two Major PFA Platforms Compare
Boston Scientific and Johnson & Johnson each offer a pulsed field ablation platform designed to work as an integrated system in the EP lab. Boston Scientific’s FARAPULSE originated at Farapulse, Inc., which the company acquired in 2021; the name echoes Michael Faraday’s legacy in electromagnetism, though no official naming explanation has been published. The platform combines a dedicated catheter, a generator with its supporting modules and cables, and a steerable sheath that helps position the catheter inside the heart. In the United States, FARAPULSE received FDA approval in late January 2024 for pulmonary-vein isolation in paroxysmal atrial fibrillation, followed by an expanded indication in July 2025 for posterior-wall ablation in persistent atrial fibrillation. Earnings reports and trade coverage link much of Boston Scientific’s recent electrophysiology growth to the system and its rapid adoption.

Johnson & Johnson’s Biosense Webster division offers the VARIPULSE Platform, which pairs the VARIPULSE catheter and the TRUPULSE generator with the company’s CARTO 3 mapping environment so therapy delivery and visualization run in a unified workflow. The platform entered the market with approvals in Japan and Europe in early 2024, which were followed by U.S. FDA approval in November. In 2025, Biosense Webster temporarily paused external use in the U.S. to review several reported neurovascular events, then resumed activity with FDA-cleared updates to labeling and irrigation-flow guidance issued in mid-July 2025.

Together, the two platforms define the current competitive landscape for PFA, with Boston emphasizing its rapid commercial momentum and J&J leveraging the established footprint of the CARTO mapping ecosystem. This rivalry also shapes how centers train and plan procedures – a natural point of connection with the growing role of high-fidelity 3D printed cardiac models.
3D Printing Opportunities in Electrophysiology
As PFA platforms move into routine practice, EP teams need faster planning, safer training, and better device evaluation. High-fidelity, patient-derived 3D models are already filling those gaps. These models shorten learning curves, standardize complex workflows, and let teams test device-plus-imaging interactions before patient care—key enablers as PFA spreads across centers.
Pre-procedural planning and case rehearsal.
Hospitals use patient-specific heart models to understand left-atrial anatomy, plan access and lesion sets, and rehearse difficult cases. Commercial offerings include Materialise HeartPrint and its scan-to-model toolchain (Mimics/Mimics InPrint) used for cardiovascular planning and printing, including left-atrial workflows.

Training and simulation for EP labs.
Printed hearts and simulators help fellows practice catheter manipulation, transseptal puncture, and ablation paths before treating patients. Recent work shows immersive simulators built on individualized 3D heart models can improve ablation performance, and open-access guides describe how to build EP ablation simulators around printed models. Vendors like HEARTROID also provide EP training models for mapping and transseptal technique.
Device testing and imaging workflows.
For labs that test catheters and energy delivery under fluoroscopy or CT, Stratasys Digital Anatomy (J850) combined with RadioMatrix produces “radio-realistic” models that appear on X-ray/CT to mimic procedural imaging. That allows dry-runs that reflect how devices will look and behave under imaging in the lab.
LAA planning alongside EP programs.
EP programs often work alongside left-atrial appendage (LAA) services. Patient-specific 3D printed atrial models and planning software (such as Materialise Enlight) help teams size and select LAA closure devices and rehearse difficult cases. BIOMODEX has created patient-specific LAA simulation stations used by major centers.
As hospitals and device makers expand their use of advanced modeling, imaging, and simulation to support PFA programs, the behind-the-scenes innovation becomes just as important as the tools physicians use in the lab. Developing patient-specific models, refining materials to mimic tissue behavior, adapting printing parameters for visibility under imaging, and integrating these models into training and evaluation workflows all require sustained engineering effort. Those activities fall squarely within the kind of process development, prototyping, and software integration work that qualifies as research and development under U.S. tax rules, creating a natural bridge to the R&D incentives available to MedTech companies and the suppliers who support them.
The Research & Development Tax Credit
The now permanent Research and Development (R&D) Tax Credit is available for companies developing new or improved products, processes and/or software.
3D printing can help boost a company’s R&D Tax Credits. Wages for technical employees creating, testing and revising 3D printed prototypes can be included as a percentage of eligible time spent for the R&D Tax Credit. Similarly, when used as a method of improving a process, time spent integrating 3D printing hardware and software counts as an eligible activity. Lastly, when used for modeling and preproduction, the costs of filaments consumed during the development process may also be recovered.
Whether it is used for creating and testing prototypes or for final production, 3D printing is a great indicator that R&D Credit eligible activities are taking place. Companies implementing this technology at any point should consider taking advantage of R&D Tax Credits.
Conclusion
As pulsed field ablation becomes a defining technology in electrophysiology, Boston Scientific and Johnson & Johnson are shaping the direction of the field through competing platforms and rapid global expansion. Their race for clinical leadership is accelerating demand for better planning, training and device-evaluation tools, areas where high-fidelity 3D printing already plays a practical role. As hospitals and manufacturers refine these workflows, the engineering behind anatomical modeling and simulation continues to qualify as meaningful research activity, opening the door for significant R&D tax incentives. In a segment evolving this quickly, those incentives can help teams innovate faster and bring safer, more predictable EP solutions to patients.