

Charles R. Goulding and Andressa Bonafe show why starting small, investing in people, and following clinical demand are the real drivers behind successful hospital-based 3D printing programs.
When Materialise convened its 3D Planning and Printing in Hospitals Forum 2025 in Leuven, Belgium, the gathering drew more than 150 healthcare professionals from across the globe, including surgeons, radiologists, and clinical engineers. The message from the two-day event was clear: 3D printing at the point of care is no longer a niche ambition of elite academic medical centers. It is becoming an operational reality for hospitals of every size.
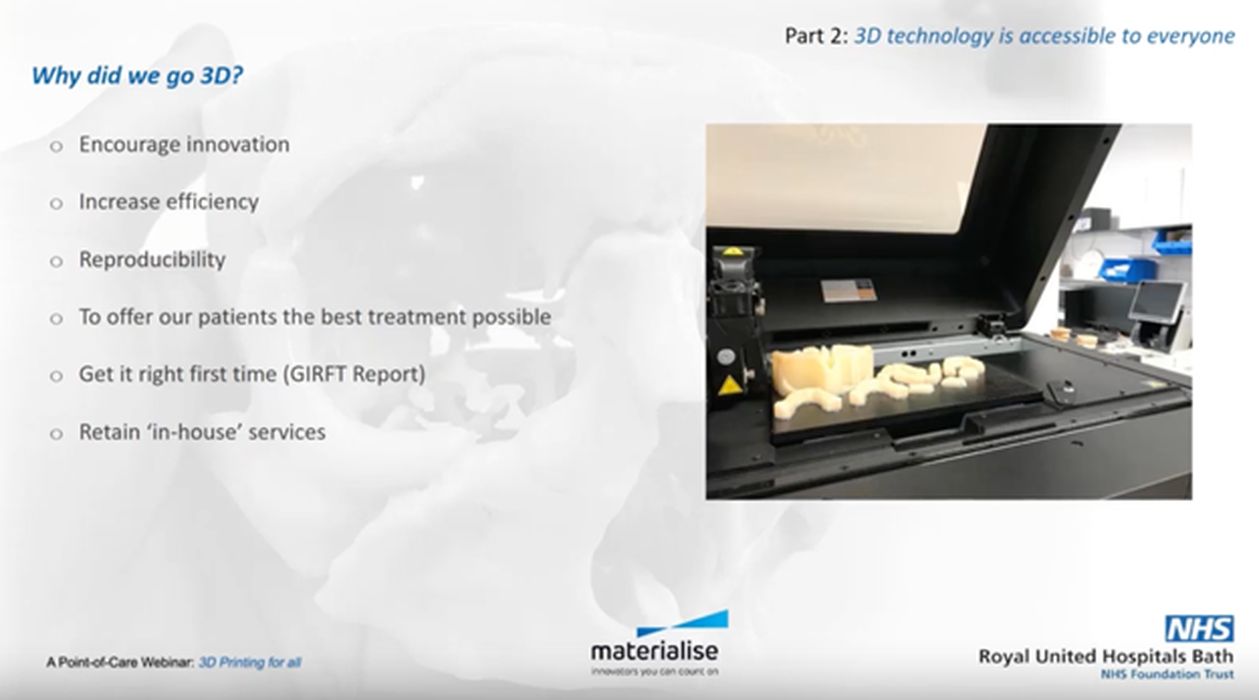
Two recent Materialise webinars put that shift into sharp focus. The first featured the oral and maxillofacial surgery team at the Royal United Hospitals Bath NHS Foundation Trust (RUH Bath), a district general hospital serving around 500,000 people in the west of England. The second featured the orthopedic team at AZ Monica Hospital in Antwerp, Belgium, whose department has spent over 15 years building one of the most advanced point-of-care 3D printing programs in Europe. The two initiatives are at different stages of the same journey. Together, they offer a practical set of lessons for any hospital considering the same path.
Start Small, Prove Value, Then Expand
Neither program began with a bold institutional vision. Both started with a specific, limited problem that 3D technology could solve, and grew from there.
At RUH Bath, the trigger was purely logistical: the department was moving to a new facility and needed to reduce its physical footprint. Digitizing a room full of plaster orthodontic casts immediately raised the question of what to do when clinicians needed physical models. That question justified the first 3D printer. Once the printer was in the building, other applications followed naturally, and what began as an orthodontic workflow tool became the foundation of a full surgical planning and point-of-care printing service.

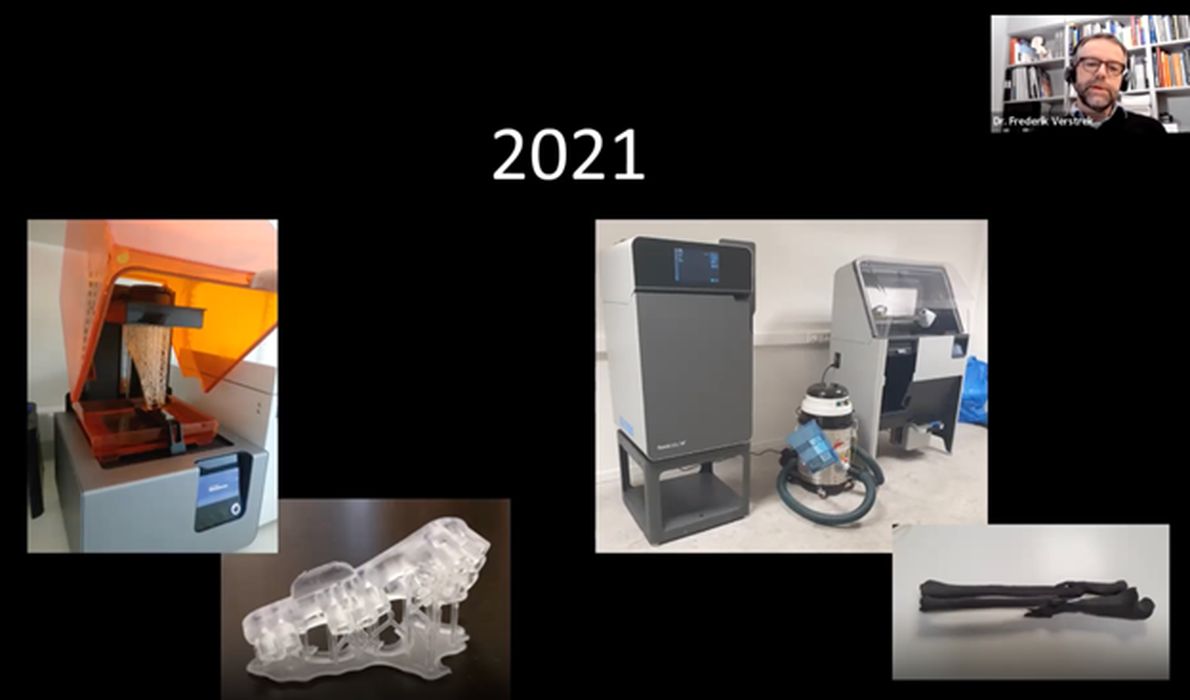
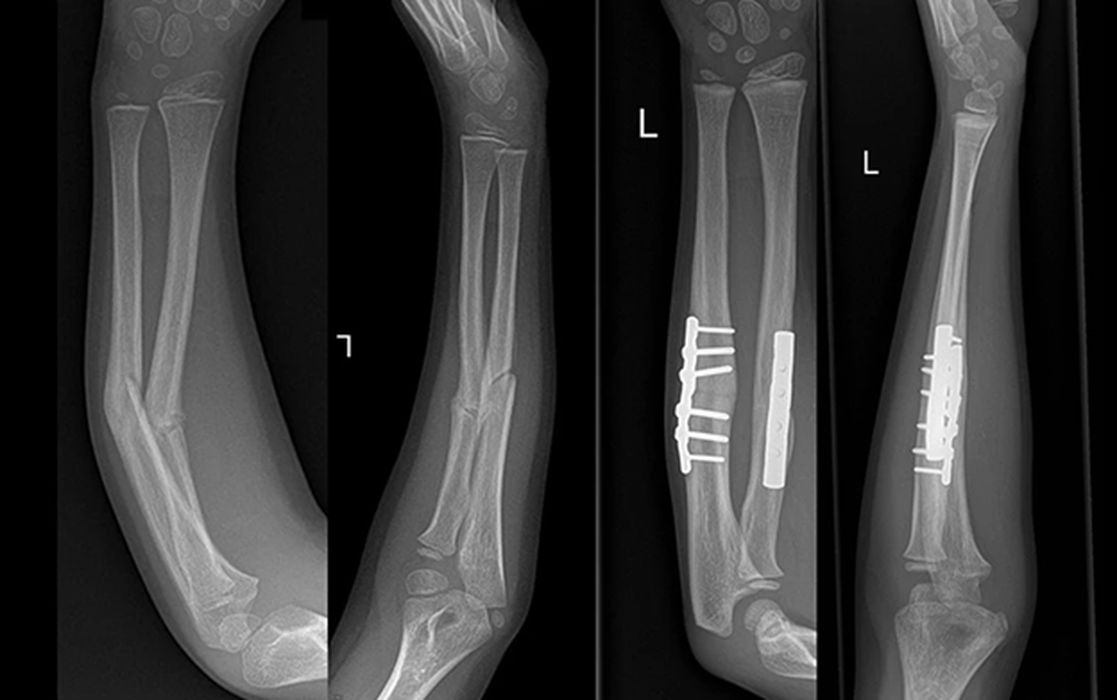
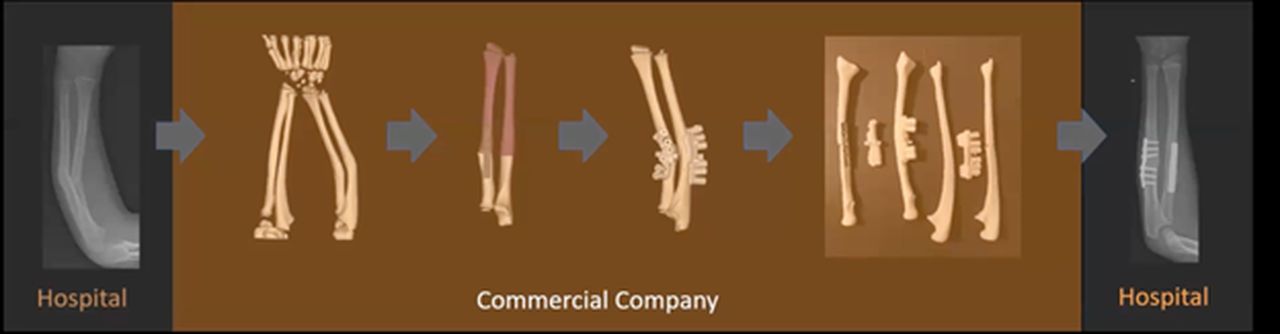
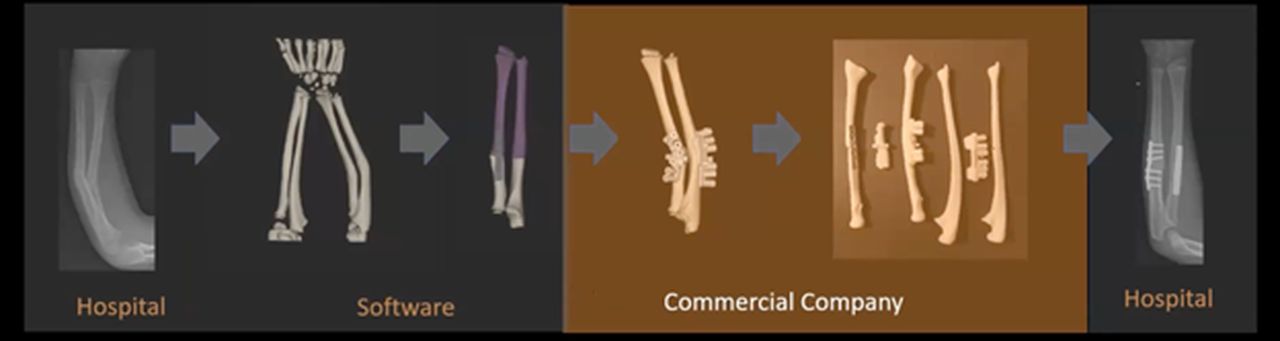
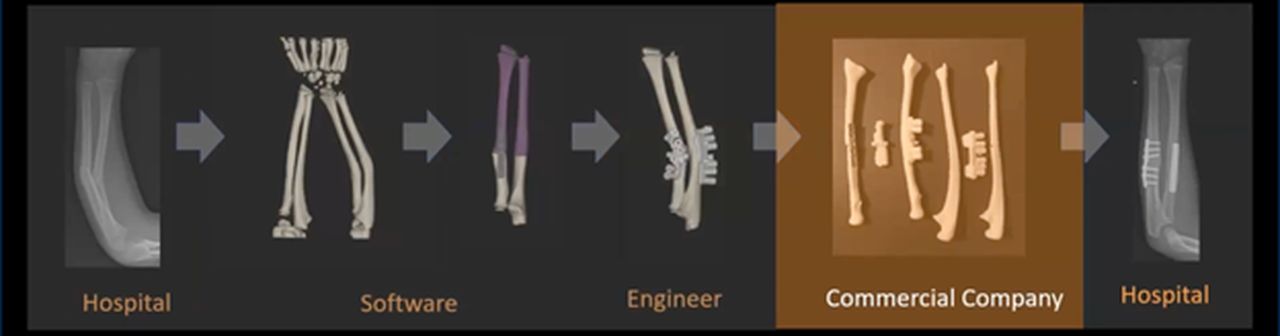
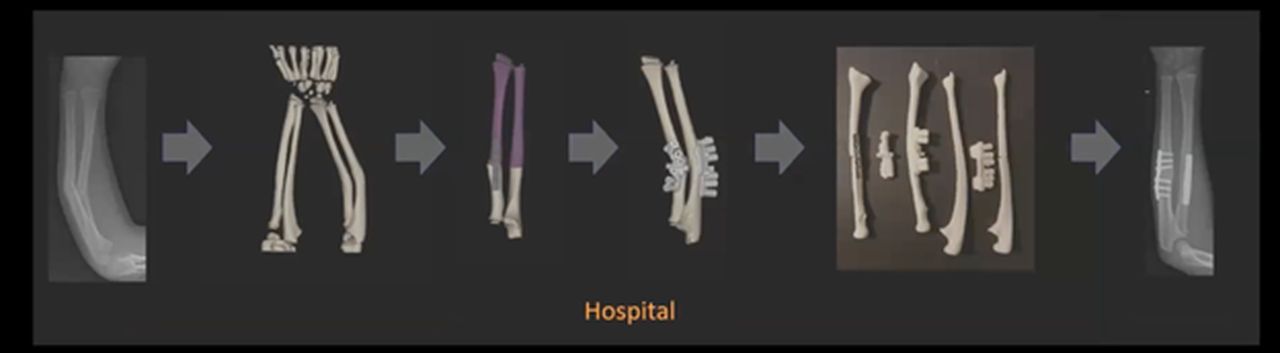
AZ Monica’s story follows the same logic over a longer arc. The department’s first 3D case, a complex malunited forearm fracture, was handled entirely by Materialise as an external partner. That collaboration worked, but it was slow. Over the following years, the hospital progressively brought each step of the workflow in-house: first the planning software, then a dedicated clinical engineer, then an SLA printer, and finally an SLS machine. At no point was the full system installed at once. Each addition was justified by the capability gap it closed. The lesson from both is the same: the business case for point-of-care 3D printing does not require a complete vision upfront. It requires one department, one problem, and one printer. The rest follows.
The Real Engine Is Human Capability
Both programs are built around a single clinical engineer or technician who serves as the operational center of the lab. At RUH Bath, the department’s digital technologist came in as an orthodontic technician with no prior experience in surgical planning software. He became a proficient user through sustained self-directed training, including completing the entire Materialise online training academy during the COVID-19 lockdown when clinical work had stopped. That period of uninterrupted learning, compressed years of gradual skill-building into a few months. The first clinical 3D printing case at the hospital came just weeks after the software was installed.
At AZ Monica, the clinical engineer hired to run the lab is described by the surgical team as instrumental to everything the department can do. The limiting factor on how many cases the lab can take on each week is not hardware, not software, and not clinical demand. It is the engineer’s available time. The department has identified more cases where 3D planning would add value than the current staffing can support.
Both programs arrived at the same conclusion independently: investing in the technical people running the lab, through training, time, and institutional support, is paramount. It is the investment that makes all other investments work.
Adoption Starts With Clinical Demand
In both cases, the adoption of 3D printing was clinician-led. The technology did not arrive as a management initiative or a procurement decision. It arrived because a surgeon saw what it could do and wanted it. At AZ Monica, the department’s lead hand surgeon saw a colleague use 3D planning on a complex case and spent roughly a year thinking through what it could mean for his own practice before committing. The tipping point was a specific patient: a malunited forearm that he recognized, without any ambiguity, could not be corrected properly using the standard two-dimensional approach. That moment of clinical necessity drove everything that followed.
At RUH Bath, the consultant maxillofacial surgeon described the shift in direct terms: the technology is genuinely game-changing, and within a short period of using it, it becomes difficult to imagine practicing without it. He now uses Materialise Mimics and ProPlan CMF for everything from complex trauma visualization to orthognathic planning and custom implant design. Among the main benefits, he highlights that bespoke 3D-printed surgical wafers fit perfectly every time, eliminating the rework and appointment cancellations that came with analog fabrication. Custom orbital implants, designed to fit a specific patient’s anatomy, go in cleanly where off-the-shelf versions required complex intraoperative adjustment.
The pattern is consistent: 3D printing programs in hospitals succeed when they are pulled by clinical demand, not pushed by technology. Motivated surgeons who can articulate what the technology does for patients are the most effective advocates a program can have, both in the operating room and in the finance department.
Compliance is the Program’s Foundation
Both programs operate under regulatory frameworks that require in-house manufactured medical devices to meet documented quality standards. In Europe, this means the EU Medical Device Regulation, which includes a hospital exemption for in-house devices, provided the device is manufactured and used within the same institution, clinical need is documented, and a quality management system (QMS) is in place. Both teams described setting up the QMS as one of the most challenging parts of the entire program.

Materialise has moved to address this directly. Mimics was the first medical imaging software to receive FDA clearance for diagnostic use in hospitals. Materialise has since built a certification program that validates specific hardware, including the Formlabs Fuse series, for use alongside Mimics. That validated combination gives hospital labs a documented basis for their quality processes rather than requiring them to construct validation evidence from scratch. The Mimics Flow Case Management platform provides the tracking and documentation infrastructure that quality systems require as caseload grows.
The practical advice from both programs is similar: engage the hospital’s regulatory and medical physics teams from the beginning, not after the printer is already running cases. The regulatory framework is workable, but it takes time to build, and the documentation burden only increases as the service expands.
The Destination Is Hospital-Wide
Both programs started in a single department. Both are now expanding, and both see the same destination: a centralized 3D printing service that any department in the hospital can access.
RUH Bath has already moved beyond its founding OMFS department. The lab now produces anatomical models for orthopedic hip revision planning, temporal bone sections for ENT surgical rehearsal, and components for medical physics clinical trials. The team’s stated ambition is an autonomous hospital-wide 3D printing department with a fleet of different printer types, each matched to the needs of a particular specialty, partly funded through private sector clinical work.
At AZ Monica, the expansion is clinical rather than departmental. While the lab’s primary focus is hand and wrist surgery, the surgical team has begun identifying additional case types across orthopedics where 3D planning could improve outcomes. Within their own practice, patient-specific surgical guides have reduced operating room time by 30 to 40 percent for eligible cases, a result that suggests broader potential as the program grows.
The economic logic supports expansion. Both programs justify their investment primarily through Operating Room (OR) time savings, reduced rework, and the ability to offer procedures that would otherwise require outsourcing or referral to specialist centers. As the service reaches more departments, that justification strengthens, and the cost of the infrastructure is shared across a broader base of clinical activity.
3D Printing as the Clinical Backbone
What makes point-of-care 3D printing particularly well-suited to this hospital-wide model is the range of technologies and materials now available at a clinical scale. Formlabs’s SLA printers produce high-resolution anatomical models and sterilizable resin guides. The Formlabs Fuse 1+, an SLS system designed for clinical environments, prints in medical-grade Nylon 12, a material that handles sterilization reliably and can produce larger parts, such as a complete forearm model, without the support structures that complicate resin workflows. Polyjet printers, used at RUH Bath, offer fine-resolution multi-material output suited to complex anatomical modeling. Together these technologies cover most of what a hospital 3D lab needs, and none of them require the footprint or capital expenditure of industrial-scale systems.

Materialise’s software platform ties it together. Mimics handles DICOM image segmentation and 3D reconstruction. ProPlan CMF supports virtual surgical planning. 3-matic handles design and print preparation. The suite is used by both hospitals featured here, and its FDA clearance and CE marking give hospital quality teams a documented regulatory foundation to build on.
The R&D Tax Credit
While the hospitals featured here are in the UK and Belgium, the technology, the workflow challenges, and the investment logic are the same everywhere. For U.S.-based medical technology companies and additive manufacturing firms developing the hardware, software, and materials that make point-of-care programs like these possible, the federal R&D Tax Credit offers a concrete financial incentive.
The now permanent R&D Tax Credit is available for companies developing new or improved products, processes and/or software.
3D printing can help boost a company’s R&D Tax Credits. Wages for technical employees creating, testing and revising 3D printed prototypes are typically eligible expenses toward the R&D Tax Credit. Similarly, when used as a method of improving a process, time spent integrating 3D printing hardware and software can also be an eligible R&D expense. Lastly, when used for modeling and preproduction, the costs of filaments consumed during the development process may also be recovered.
Whether it is used for creating and testing prototypes or for final production, 3D printing is a great indicator that R&D Credit-eligible activities are taking place. Companies implementing this technology at any point should consider taking advantage of R&D Tax Credits.
Conclusion
The programs at RUH Bath and AZ Monica Hospital make the same argument from different starting points: point-of-care 3D printing is not a project for hospitals with unlimited resources, and it is not a project that requires a perfect plan before the first printer is switched on. It requires a clinical problem, motivated surgeons, skilled technicians, and the institutional will to build quality into the process from the beginning. The technology, from Materialise’s software suite to the Formlabs’ hardware platform, exists at a scale and price point that makes this achievable for district general hospitals as much as academic medical centers.