
Researchers used 3D printed tooling to create dissolving microneedles that deliver drugs through the cheek.
Microneedle patches have been inching toward mainstream drug delivery for years, promising painless administration and simplified logistics compared to injections. The “buccal route” — through the inner cheek — also avoids first pass metabolism, a known barrier to consistent oral uptake of certain drugs. In a new study in Micromachines, the team reports dissolving microneedle (DMN) arrays fabricated with the aid of 3D printed master molds, a path that could put additive manufacturing squarely into the drug-device supply chain.
The approach combines two established ideas: use resin 3D printing to rapidly prototype sub-millimeter needle geometries, then replicate them as dissolvable polymer arrays loaded with API. That hybrid model has been gaining traction because it bypasses costly microfabrication steps and lets researchers iterate quickly on tip sharpness, base thickness, and array pitch. The benefits are clear: desktop SLA or DLP printers can deliver high-resolution molds quickly, with design tweaks pushed from CAD to mold in hours rather than weeks.
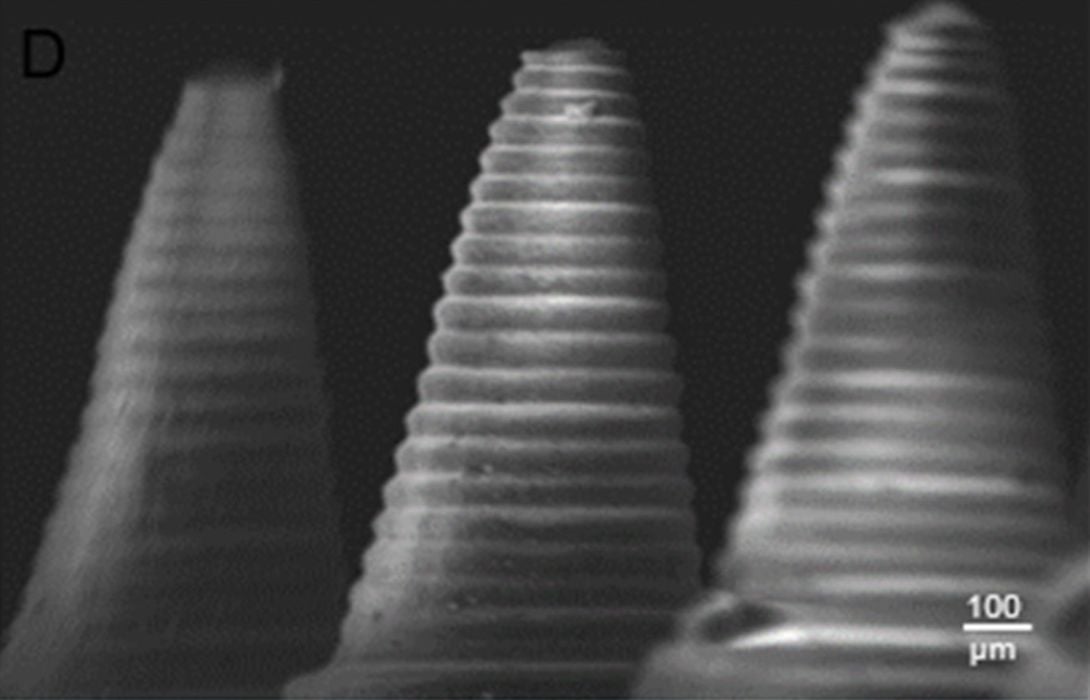
The paper describes standard characterization for this class of device: morphology and dimensions, mechanical strength and insertion performance in tissue, dissolution behavior, and in vitro permeation. Their proposed platform’s logic extends to many small molecules and biologics that could benefit from transmucosal delivery. The master molds are the additive piece; once qualified, they enable repeatable micromolding runs without exposing patients to any printed resin.
Mechanism and Materials
The DMNs are typically formed from water-soluble, biocompatible polymers such as polyvinylpyrrolidone or polyvinyl alcohol, with plasticizers to balance brittleness and dissolution rate. Expect the formulation to include surfactants or carriers to keep drug uniformly distributed and bioavailable. This is where additive-enabled rapid screening matters: swapping polymer grades, needle heights and base thicknesses can be done across a design matrix and printed into new masters quickly, all to match with the formulations.
SLA or DLP resolution, surface finish and post-processing are the main constraints. Tip radii and wall smoothness affect insertion force and pain perception, while stray resin or inadequate post-cure can create defects in the mold. The study does not state printer model or layer thickness in the abstract-level information we reviewed, and so their exact throughput is unknown. Nevertheless, compared with silicon or lithographic routes, the CAPEX and lead time advantages are clear, especially for labs or startups exploring niche doses or personalized patches.
Economically, the combination could reduce labor and inventory. A service bureau or hospital pharmacy could keep validated master sets and cast on demand, adjusting array dimensions or load to patient need. Quality systems are unmentioned: dose uniformity, polymer moisture uptake, and shelf-life stability must be locked down before any of this could be commercialized. Sterilization compatibility — gamma, ethylene oxide or aseptic build — can change polymer properties, and the paper does not seem to address a production sterilization protocol.
Who Benefits, And What’s Missing
Dental and oral-medicine clinics, pain and neurology practices, and compounding pharmacies might see immediate value if clinical performance bears out. AM’s role would be in low-volume, high-mix tooling and possibly semi-automated casting jigs, not direct patient-contact prints. For larger scales, injection or roll-to-roll microreplication could pick up once designs stabilize, with 3D printing staying upstream for rapid design control and tech transfer.
If 3D printed masters can turn microneedles from mere prototypes into repeatable, tunable products, the cheek may become one of AM’s more unexpected production interfaces.
Via Micromachines