
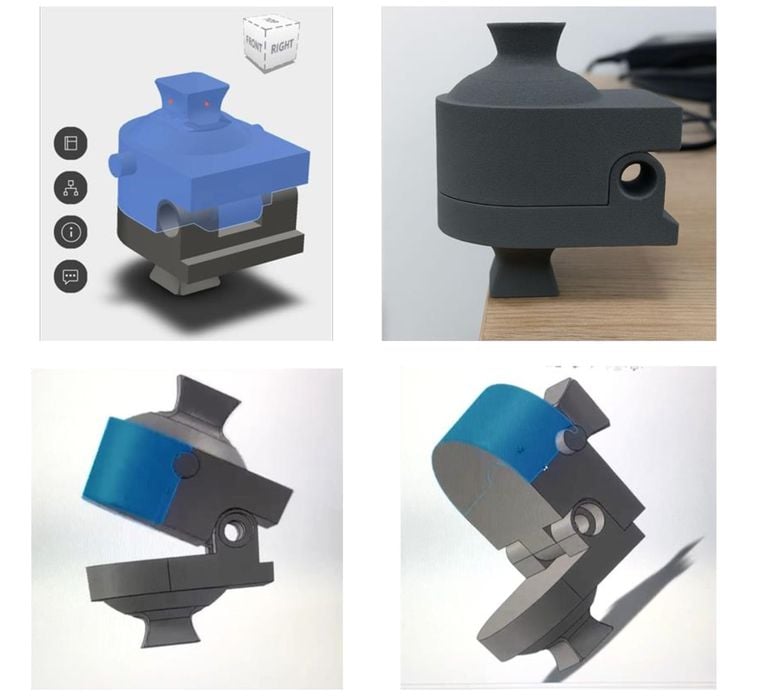
A research paper describes the “Pedi-knee”, a 3D printed prototype of a pediatric knee joint.
Additive manufacturing has already made major progress in medicine, particularly for adult patients. We have 3D printed anatomical models, surgical guides, dental devices, titanium implants, and an increasing number of patient-specific tools.
But children are not just small adults. That is the problem Pedi-knee appears to address.
A child’s knee is a much more complicated design target than an adult knee. The bones are smaller, obviously, but they are also still growing. Growth plates remain open. Cartilage, ligaments, and soft tissues are changing. Alignment can shift as the child develops.
In other words, scaling down an adult knee model is just not good enough.
That makes pediatric biomechanics a difficult area for engineers, surgeons, and medical device developers. They need models that represent child-sized anatomy, but also models that behave in a useful mechanical way.
That seems to be where Pedi-knee fits.
It appears to be a working joint prototype, which is far more interesting than just a concept. They actually made one of these.
Static 3D printed models are already used in pediatric surgery planning. A surgeon can look at a child-specific bone structure before entering the operating room, and that can be quite useful.
But a moving joint is another level of difficulty.
A knee is not just a shape. It is a set of interacting surfaces, ligaments, constraints, clearances, loads, and motions. If a 3D printed model is intended to reproduce some of that behavior, then the design challenge becomes much harder.
The potential payoff is also much larger.
A reliable pediatric knee surrogate could help with training, surgical planning, device design, and perhaps early bench testing of pediatric orthopedic concepts. That is beneficial because pediatric medical devices are often hard to commercially justify. The patient population is smaller, the anatomy varies widely, and testing is complicated.
A low-cost, reproducible model could lower that barrier.
But there’s one issue: We need to know what kind of model this actually is. Is Pedi-knee primarily an educational demonstrator? Is it a simulator fixture? Is it intended for surgical rehearsal? Or is it a step toward preclinical device testing?
For example, SLA or DLP printing could produce high-resolution joint surfaces, which would be useful for representing cartilage-like geometry. FFF could produce tougher or more flexible parts, particularly if TPU is used for ligament-like elements. SLS nylon might offer a good balance of durability and print fidelity.
If the goal were implant realism, then materials like PEEK or metal AM would enter the discussion. But for simulation, education, and early research, multi-material polymers are probably the more practical route.
The interesting AM challenge here is not printing a knee-shaped object, instead it is 3D printing a joint that moves predictably and accurately according to actual human joint behavior.
That means controlling surface finish, friction, stiffness, wear, and alignment. It also means thinking about replacement parts. A useful test model might need swappable ligaments, menisci, or contact surfaces so that researchers can represent different ages, injuries, or pathologies.
That is where additive manufacturing could be genuinely useful.
A conventional manufactured model might be expensive and fixed in its geometry. A 3D printed model could be modified quickly, printed in multiple sizes, and adapted for different scenarios. That is exactly the kind of low-volume, high-variation problem where additive approaches usually makes sense.
A teaching model only needs to look and move plausibly.
A simulator model needs to behave consistently.
A preclinical test platform needs validation.
Those are not the same thing.
Cost and accessibility could become major advantages. If Pedi-knee can be printed using common polymer systems and open materials, then children’s hospitals, university labs, and orthopedic researchers could potentially reproduce it locally.
That would be important.
Pediatric research is not always well-funded, and many useful ideas fail because the tooling is too expensive or too specialized.
But if the model depends on proprietary resins, closed software, or difficult post-processing, adoption will be much narrower. That would limit its impact, especially in lower-resource settings where pediatric orthopedic tools may be badly needed.
For clinicians, a robust pediatric knee model could help explain procedures, rehearse unusual cases, or plan adolescent ligament reconstructions and osteotomies.
For device makers, it could provide a faster way to iterate across sizes and growth stages.
For service bureaus, it could become a small but interesting niche: custom pediatric joint models for hospitals and research teams.
The real opportunity would be a parametric design.
Imagine a printable pediatric knee platform where age, size, alignment, and pathology could be adjusted in CAD, then printed as needed. That would be much more powerful than a single fixed prototype. But there’s a lot of work ahead before that happens.
The Pedi-knee could become a practical reference platform for pediatric knee research and training. That would be a good use of additive manufacturing: not hype, not novelty, but a way to make a difficult, variable, low-volume medical problem easier to study.
Adult knees are hard enough. Growing knees are a moving target.
Via OpenAlex