

Charles R. Goulding and Andressa Bonafe detail the R&D tax credit implications for medical device innovators who overcome manufacturing uncertainties to produce unique brackets individualized across six distinct dimensions.
On April 28, 2026, LightForce Orthodontics announced LightBracket Metal, a patient-specific 3D printed metal bracket generated from an orthodontist’s digital treatment plan. The company describes the launch as an expansion of its “generative braces” system, in which the treatment plan becomes the input and the bracket becomes the output. Rather than relying on standardized brackets selected from a catalog, each LightBracket Metal appliance is generated and manufactured for a specific patient and a specific tooth.
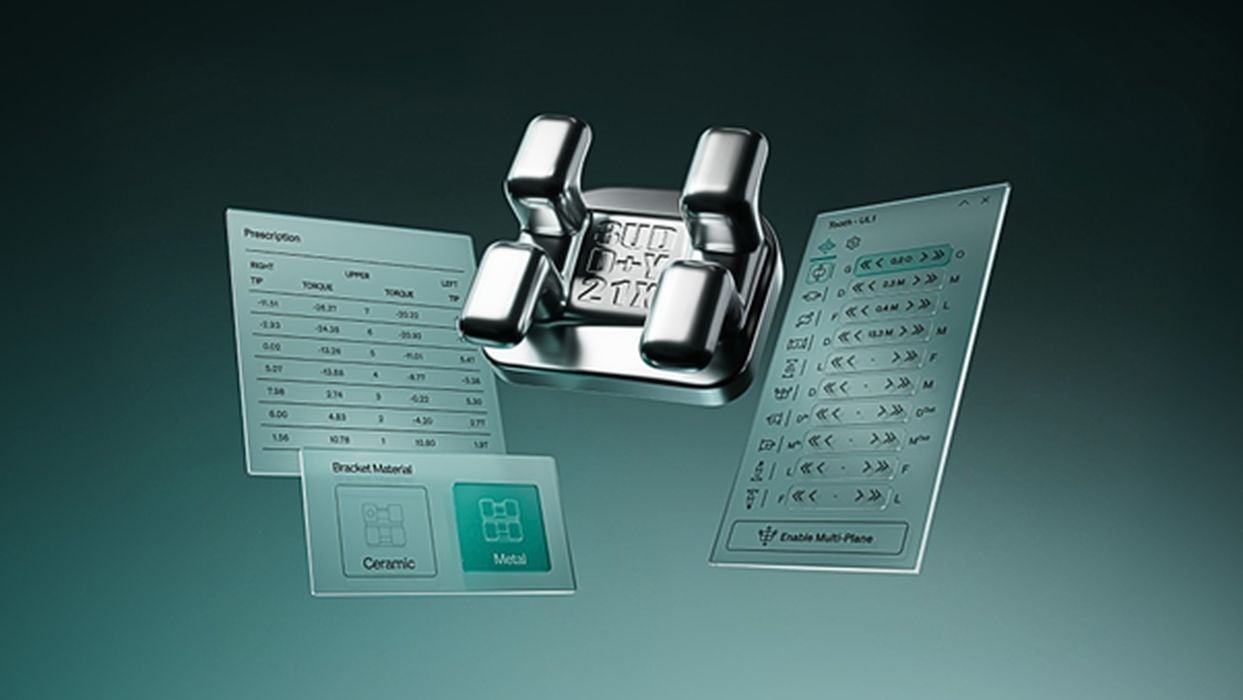
The launch matters because metal remains central to orthodontics. According to LightForce, 65% of orthodontic patients worldwide choose metal braces, including many teenagers. The new product extends LightForce’s individualized bracket approach beyond its original ceramic system and into the largest segment of fixed orthodontic treatment. LightBracket Metal is produced using a proprietary 3D metal printing process and is individualized across six dimensions, including bracket base, slot height, slot prescription, bracket position, tie wings, and hooks.
The broader market context is also significant. MarketsandMarkets projects the global orthodontic supplies market to grow from US$7.17 billion in 2025 to US$10.96 billion by 2030, reflecting continued demand for orthodontic products and treatment systems. For additive manufacturing, LightBracket Metal is an example of how 3D printing can move beyond prototyping and into high-volume, patient-specific medical device production.
To better understand the launch and its implications for orthodontics, 3D printing, and personalized manufacturing, we spoke with James Lawton, President of LightForce Orthodontics.

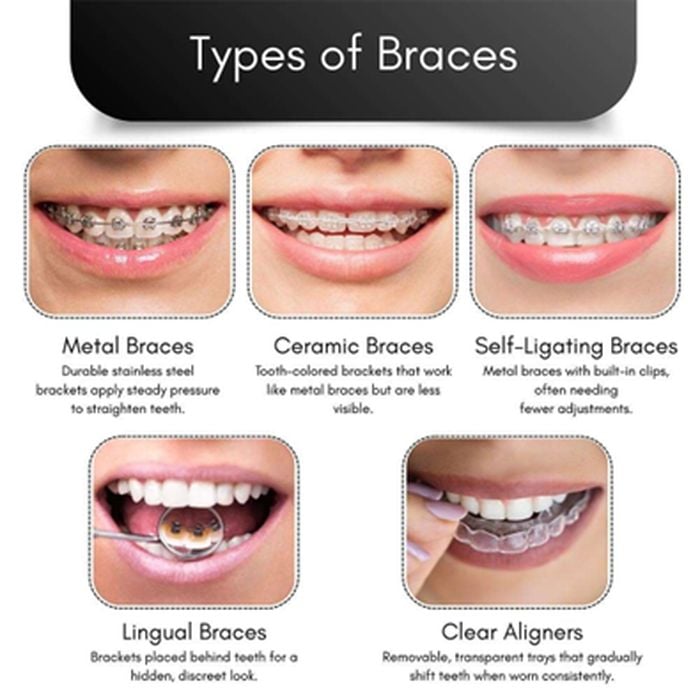
LightBracket Metal is being described as bringing the clear aligner-style personalized experience to braces patients. What does that shift mean for orthodontics, especially in a market where metal braces remain so widely used?
If you think about the braces someone gets today, they are a lot like the braces I got, the braces my father got, and even the braces my grandfather got. Essentially, the way braces have worked for decades is through a catalog. Orthodontists have a handful of stock brackets to choose from.
The orthodontist places those brackets on the teeth, bends the wire in a way they think will move the teeth closer to the desired position, and then the patient comes back six weeks later. At that point, the orthodontist evaluates what moved as expected, what did not, and bends another wire. In many ways, it becomes a series of iterative experiments using standard brackets.
Teeth are a lot like fingerprints. They are unique to the person. That is why people can be recognized through dental records. The idea with LightForce is to start with the end in mind. Orthodontists think about that as the finish: what the smile is ultimately going to look like.
From there, the bracket is designed for that specific patient’s tooth and for the smile the orthodontist is trying to create. The goal is to provide the best possible clinical outcome with the fastest possible treatment time, because the teeth are moving more directly from where they are to where they need to go.
That is similar to what aligners introduced: the digitization of a process that was historically more manual and more experimental. The difference is that metal braces are still widely used, especially among teenagers. Teenagers’ teeth may not be fully erupted yet, or they may be rotated, crowded, or positioned unusually. Being able to uniquely grab that tooth and move it efficiently is much more effective when the bracket is designed for that specific application rather than selected from a catalog.
Today, 65% of the market uses metal. Metal is a material orthodontists know and like, and it is also preferred by many teenagers.
LightForce pioneered fully customized 3D printed ceramic brackets. What technical or manufacturing challenges had to be solved to extend that personalized model into metal brackets?
We benefited from having developed some of the core processes earlier. The company has been around since 2019, and initially our 3D printed brackets were available only in ceramic. That taught us a lot about the technology and allowed us to progress through the creation of the metal equivalent more quickly. The metal system took on the order of a couple of years, compared with the longer development period for ceramic.
One of the biggest variables is that we have hundreds of patient-specific bracket designs on the floor at any given time. Every bracket is made once, for that tooth, for that patient. Building a robust, reliable, repeatable manufacturing process that can handle hundreds of thousands of brackets at any given time is complicated.
A significant technical challenge was choosing the right technology. There are many different 3D printing technologies, and we intentionally chose digital light processing because of its ability to provide resolution, which directly drives precision. These are not big parts, so the precision with which you make them affects how effective the treatment is and how quickly it can progress.
Repeatability is also critical because there is such a wide variety of parts being manufactured. Then there is the challenge of scale: how do you get the throughput needed to cost-effectively provide a unique bracket for an individual patient? That comes down to the choice of technology and how that technology is applied specifically to custom braces.
There is also the software behind the manufacturing process. We start with the patient’s anatomy, the desired outcome, and the treatment plan. The software uses that information to design a specific bracket, which then goes through a slicer and into the 3D printing process.
The term “generative braces” suggests that the appliance is created directly from the treatment plan rather than selected from stock parts. How should orthodontists understand this concept, and how does it change the relationship between software, hardware, and clinical decision-making?
The simplest way to think about it is this: no bracket exists until the patient does. The treatment plan and the patient data are the input. The brackets are the output. The appliance is created directly from the doctor’s plan, made for that one patient, and not selected from a catalog.
Today, with stock brackets, the orthodontist assesses the patient, chooses a bracket from a catalog, and typically applies that bracket at the FA point, the facial axis, roughly centered vertically and horizontally. From there, the orthodontist bends the wire to try to achieve the desired outcome. Each visit requires the orthodontist to perform that work.
With a software-enabled digital process, the doctor defines the final end state, or what they want the finish to look like. With the help of software, we create the brackets.
Those brackets are then loaded into trays that are also uniquely designed for the patient. When the tray is inserted into the mouth and the bracket is adhered to the tooth, there is only one place where that bracket can go. It is the optimal place to reach the final outcome.
That does two things. First, it increases the likelihood of better outcomes because the bracket placement is highly precise. Second, it changes the operational workflow inside the orthodontic office.
The most valuable and expensive asset in any orthodontist’s office is the orthodontist. If the orthodontist has to apply every bracket manually, the process for one patient can take 90 minutes to two hours. With bonding trays, the trays function almost like manufacturing jigs. There is only one place the brackets can go.
That means the broader clinical staff can perform bonding, while the orthodontist oversees multiple bonding appointments at the same time. From my background in robotics, I think of it as a workforce multiplier. The orthodontist can leverage their expertise across multiple patients because the clinical staff can rely on the software and the uniquely designed parts.
From a manufacturing standpoint, what makes 3D printing especially well suited to orthodontic brackets, where every patient and every tooth can require a slightly different geometry?
The process begins with a digital scan of the mouth, using a device that looks a lot like an electric toothbrush. That scan creates a digital view of the patient’s teeth.
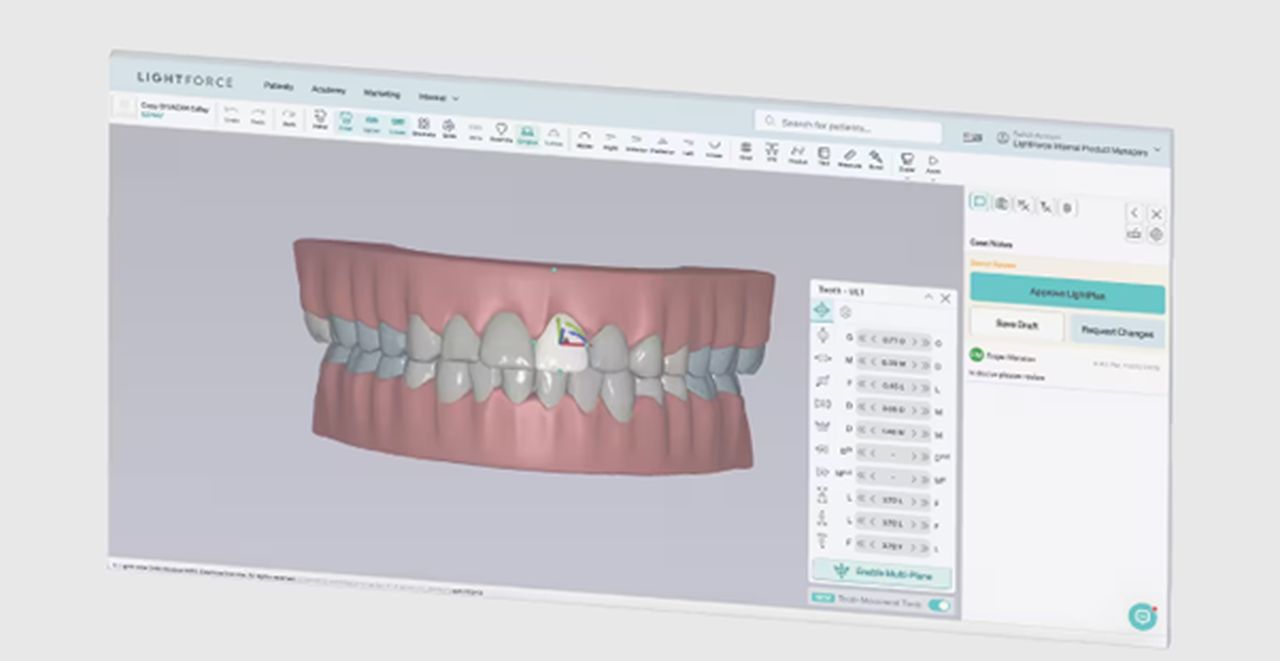
Our planning software uses that scan as the starting point. The doctor has preferences about what the final position should look like, and the software creates the bracket. The bracket is then handed off into the manufacturing system.
We do the printing ourselves. The brackets are generated by our 3D printers, and then the braces are inserted into trays, which are also 3D printed. So the unique brackets go into unique trays, and that combination is what gets sent to the orthodontist.
This is a case where form meets function. Teeth are unique, and there really is not another process we could use that would allow us to create a unique bracket cost-effectively and with a biocompatible material. Bringing those three things together is what makes 3D printing the enabling technology. Without it, we could not do this.
Clinical efficiency is a major part of the LightForce story, including fewer appointments and shorter treatment times in published studies. As LightBracket Metal scales to a larger share of cases, what evidence or real-world metrics will matter most in showing orthodontists that customization changes outcomes?
The numbers that matter are clinical outcomes, treatment time, appointments, and the amount of wire adjustment required.
With LightForce, we have seen 60% fewer appointments, 43% shorter treatment time, and 70% fewer wire adjustments. These numbers come from third-party, independent, peer-reviewed clinical journals.

In practical terms, if a patient would normally spend about two years in braces, that can move closer to roughly one year. With fewer wire adjustments, the orthodontist can put on a straight wire, attach it to the braces, and allow the system to do more of the work. That reduces the amount of manual wire bending typically involved.
There are also studies demonstrating that the quality of the outcome is higher. The final finish can be closer to ideal than with manual stock brackets.
Looking ahead, where do you see personalized orthodontics evolving over the next five to ten years? Do you expect the industry to move steadily away from stock appliances toward fully customized, software-driven treatments, and what role will 3D printing play in that transition?
Generative braces are the next era in personalized orthodontics.
I think the model we will see five years from now is that there will be two systems used in orthodontics, and both will be digitally enabled around customization: aligners and generative braces.
The advantage of having those two systems in an orthodontic practice is that the workflows are very similar. They are both digital, and they both have approximately the same amount of time between visits. That allows practices to optimize how they operate.
Aligners are generally favored more for adults. With teenagers, compliance can be a challenge because aligners have to be worn around 22 hours a day. There are also certain things braces can do that aligners have a harder time doing. Aligners can push teeth, but because they are not actually holding on to the tooth, pulling teeth can be more difficult. If you need to move a tooth forward, you often want a bracket so you can get a grip on the tooth.
Ultimately, I think we reach a point where stock brackets are no longer the standard. Instead, orthodontics will rely on digitally enabled aligners and digitally enabled generative brackets.
That shift is also a scaling challenge. I was brought into LightForce because I have experience at Walmart, Hewlett Packard, and other large companies scaling technologies. The idea behind LightForce is relatively simple, but making it happen at scale is really hard.
We use 3D printing, computer vision, robotics, and automation. Figuring out when to apply each technology, and at which process step, is what makes or breaks the ability to do this at scale. That combination of technologies is what will allow us to produce these systems in the millions over the next few years.
| Industry | Innovation | Clinical Impact |
| Orthodontics | 3D Printed Generative Brackets | 60% fewer appointments |
| Orthodontics | Patient-Specific Bonding Trays | 43% shorter treatment time |
| Orthodontics | Software-Driven Planning | 70% fewer wire adjustments |
How LightForce Orthodontics’ 3D Printed Metal Brackets Qualify for R&D Tax Credits
Companies developing patient-specific medical devices, such as LightForce Orthodontics’ LightBracket Metal, can claim the Section 41 R&D Tax Credit for expenses related to the systematic elimination of technical uncertainty in additive manufacturing. Qualifying activities include the development of proprietary 3D metal printing processes, the integration of digital light processing (DLP) for high-resolution precision, and the creation of automated software workflows that translate digital treatment plans into individualized bracket geometries. These innovations move 3D printing beyond prototyping into high-volume, personalized healthcare production.
What makes LightBracket Metal technically unique for R&D purposes?
Unlike traditional mass production, where one design is manufactured many times, LightForce must repeatedly produce individualized parts while maintaining strict quality and cost efficiency. Each bracket is generated across six unique dimensions: bracket base, slot height, slot prescription, bracket position, tie wings, and hooks. This “generative” approach—where treatment plans serve as the direct input for manufacturing—requires continuous experimentation with print resolution, material repeatability, and software-driven geometries.
Which activities qualify for the Section 41 R&D Tax Credit?
Development projects that satisfy the IRS Four-Part Test—specifically those involving technical uncertainty and iterative testing—are eligible. In the context of 3D printed orthodontics, qualifying work includes:
· Process Improvement: Developing robust, repeatable manufacturing processes capable of handling hundreds of thousands of unique bracket designs simultaneously.
· Software Integration: Building custom software and “slicers” to convert patient anatomy and orthodontic end-states into manufacturable 3D files.
· Automation & Robotics: Integrating computer vision and robotics to scale personalized production and function as a “workforce multiplier” in clinical settings.
· Material Science: Testing biocompatible materials and alternative metal printing technologies to ensure clinical efficacy and patient safety.
The LightForce example is especially relevant because each bracket is unique. That creates a different technical challenge than traditional mass production. Instead of making one design many times, the company must repeatedly manufacture individualized parts while maintaining quality, accuracy, and cost efficiency. Solving that kind of uncertainty often requires systematic experimentation, which is a key feature of qualifying R&D activity.
Orthodontic practices and manufacturers adopting or developing digital workflows should also consider whether their work involves process improvement, software integration, or new clinical production methods. Not every implementation activity will qualify, but projects that involve technical uncertainty, iterative testing, and the development of new or improved products or processes may be eligible for valuable federal and state R&D Tax Credits.
Conclusion
LightBracket Metal represents more than a new bracket material. It marks an effort to bring fully customized, digitally planned, 3D printed orthodontics into the metal braces segment, where a large share of patients still receive treatment. As Lawton emphasized, 3D printing is the enabling technology that makes patient-specific brackets possible at scale, but the broader story also includes software, automation, clinical workflow, and practice efficiency. The launch is another example of additive manufacturing moving into high-volume personalized healthcare applications, with clear implications for innovation strategy and potential R&D Tax Credit eligibility.