
A new academic roadmap lays out how orthopedic 3D printing could evolve into clinical bioprinting by 2050 — and what must happen along the way.
Authored by Lucian Reclaru and colleagues from Switzerland and Romania, the paper contrasts subtractive CAD/CAM with additive methods and projects an orthopedic future that moves from patient-matched titanium lattices to living, vascularized grafts. This is a state-of-the-field analysis with a strong forecast.
They synthesize three decades of AM development — from stereolithography to laser powder bed fusion — and connect it to real orthopedic practice and near-term hospital workflows.
Their premise is straightforward. Subtractive CAD/CAM remains excellent for hard, precise components, but wastes material and limits internal geometry. Additive manufacturing enables porous lattices, tuned stiffness, and true patient specificity. In orthopedics, that means better osseointegration and potentially fewer attachments.
Orthopedics Moves From Milling To Lattices
The review tracks the usual AM technologies: Selective Laser Sintering and Melting (SLS/SLM), Direct Metal Laser Sintering (DMLS), Electron Beam Melting (EBM), photopolymerization (SLA, DLP), and extrusion such as Fused Filament Fabrication (FFF) and Direct Ink Writing (DIW).
Today porous structures from LPBF and EBM are now routine in acetabular cups and spinal cages. EOS is cited for vertebral and hip work, GE Additive’s EBM for titanium implants, and Fraunhofer ILT for research into bioresorbables like calcium phosphate and polylactide. ConforMIS’s personalized knees — now within restor3d — are given as a clinical data point that customization can match or beat standard sets.
But there is one issue. The same features that make AM compelling — heat cycles, supports, thin struts — also raise risks: residual stress, surface roughness, internal porosity and variable fatigue behavior. Long-term validation is still sparse across indications, and standards lag practice. The paper is quite clear that AM’s design freedom does not remove qualification requirements.
Bioprinting Steps Toward Living Implants
The second half of the paper looks beyond metal to cells and matrices. Three bioprinting routes are summarized: biomimetic architectures, cellular self-assembly, and modular functional tissues. Industry examples range from Organovo — noted by the authors as now known as VivoSim Labs — in liver and kidney tissues, to the Wallenberg Wood Science Center’s printed ear cartilage, and Poietis in skin (reportedly inactive since 2025).
The vision for 2030–2050 is ambitious. The authors expect vascularized, partially functional organs, hybrid implants that merge titanium scaffolds with a patient’s osteoblasts, and even in situ robotic bioprinting for skin, bone and cartilage. Digital twins and AI would simulate organ mechanics before printing, while decentralized, on-demand manufacturing could reroute supply chains.
What It Means For Hospitals And OEMs
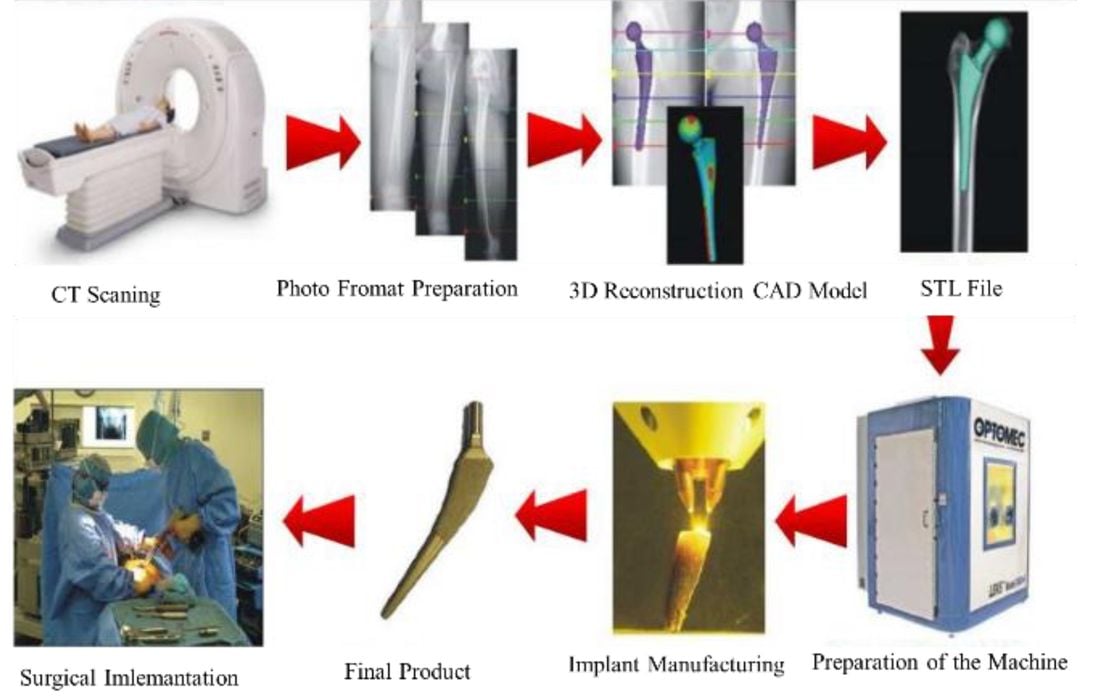
For providers, the near-term takeaway is pretty clear: by the end of this decade, expect AM to be routine for surgical planning, patient-specific guides, and a growing list of personalized implants. That implies tighter imaging-to-CAD workflows, validated lattices, and traceable post-processing and heat treatment. Throughput and labor — especially support removal and finishing — will still determine cost per case.
For equipment manufacturers, the path forward becomes more clear: automation, sensing and closed-loop control that stabilize surface condition and fatigue properties will win. Materials that balance stiffness, corrosion and osteoconductivity will become more important. And if bioprinting jumps from lab to clinic, partnerships with cell therapy, GMP facilities and imaging-robotics integration will be critical.
None of this has happened… at least not yet. But the researchers have laid out how the scene will likely play out.